22836 CARCINOMA OF THE BREAST
The patient was a woman aged 51 who presented with tenderness and firmness of the right breast for a year. She had also noticed that the breasts were of a different shape when she bent forward. The right breast had become progressively larger and two weeks before admission she became breathless on exertion and developed a cough. X-ray showed right pleural effusion and metastases in the lumbar spine and in the upper ends of both femora. Bilateral oophorectomy was performed but she died suddenly two days later. At post-mortem there was a carcinoma of the right breast with extension into the right pleural cavity and involvement of right axillary, mediastinal, coeliac, and hepatic lymph nodes, and metastases in the liver, spine and each femur.
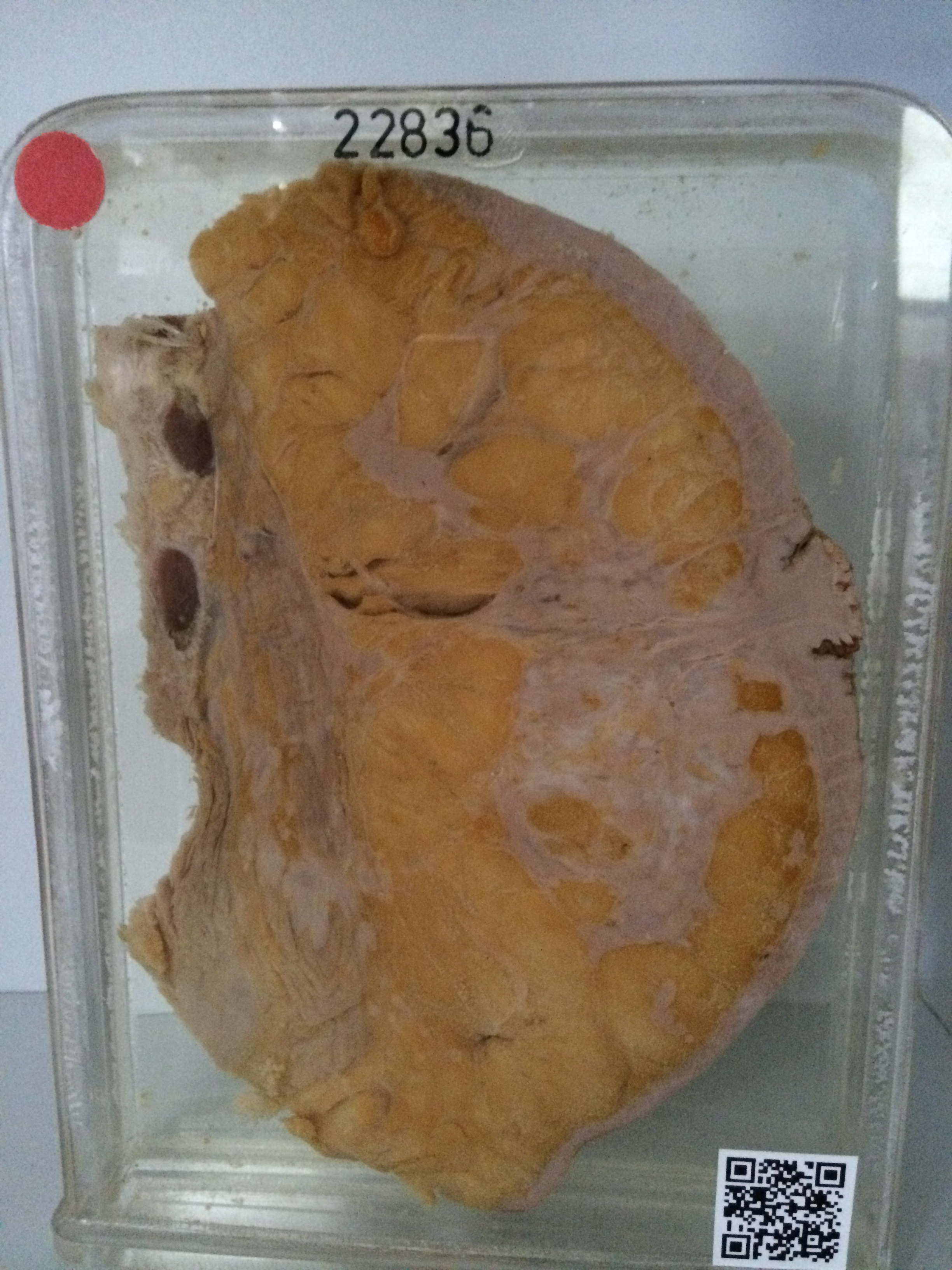
Specimen A is the sectioned breast with the underlying pectoral muscle. A large carcinoma 7 cms in diameter lies beneath the nipple which is markedly retracted. There are obvious extensions of the tumour through the fat of the breast and into the substance of the underlying pectoral muscle. A wide zone of skin around the nipple is also invaded and there is superficial crusting and excoriation, most evident in the nipple itself. Histology shows a large polygonal-celled anaplastic carcinoma extending up to the surface. The overlying epidermis is stretched.
Specimen B shows the sectioned breast, pectoral muscle, ribs and the underlying lung. As this is the other face of the specimen, the breast shows the same appearances as in 22836 A. Beneath the pectoral muscle is a large mass of tumour extending through the intercostal spaces to the pleural cavity. Almost the entire pleural cavity is filled with a thick pale layer of tumour. There has been some fibrinous pleural reaction to the presence of tumour on the parietal layer. This is most evident over the posterior and inferior surfaces of the lower lobe.