25211 ANEURYSMS OF THE DESCENDING THORACIC AORTA
The patient was a woman aged 83 who had a 6-week history of congestive cardiac failure uncontrolled with digitalis, digoxin and frusemide. She was hypertensive (240/120). Chest X-ray showed dilatation of the aorta, a right apical pulmonary opacity and emphysema. There were 23,000 leucocytes in the blood, 91% neutrophils. The right leg was swollen. Postmortem showed a carcinoma in the tail of the pancreas with secondaries in the liver, and recent antemortem thrombus in the right saphenous vein and the left internal jugular vein, extending through the innominate vein into the origin of the superior vena cava. There was a large recent infarct in the spleen.
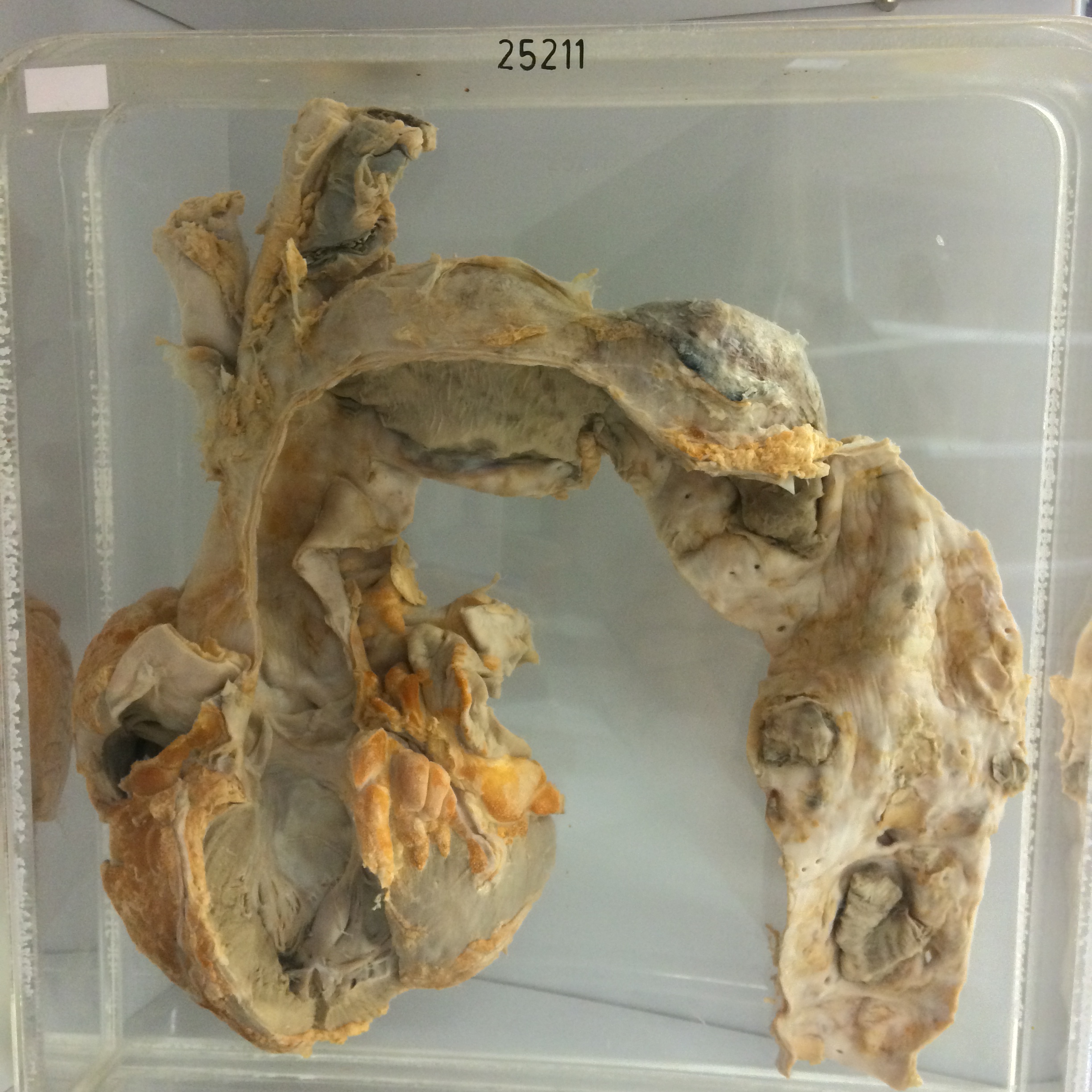
The specimen consists of the heart together with the arch and the greater portion of the descending aorta. The arch of the aorta shows considerable fusiform dilatation with some longitudinal wrinkling of the intima. There are two adjacent saccular aneurysms on the left posterolateral surface of the aorta. The proximal aneurysm measures 8 cms in length and originates just distal to the origin of the left subclavian artery. It bulges approximately 2 cms from the general line of the aorta. The distal aneurysm is about 7 cms in length and also bulges from the left postero-lateral surface of the aorta. These aneurysms are filled with dense laminated thrombus showing prominent lines of Zahn at the surface. The intima of the descending aorta distal to the 2nd aneurysm shows gross ulcerated and calcific atherosclerosis. Two large masses of antemortem thrombus are present on ulcerated plaques. The aortic valve leaflets are normal. The left ventricle is not dilated or hypertrophied. Recent antemortem thrombus is present in the left internal jugular vein and the origin of the innominate vein.