22376 SYSTEMIC SCLEROSIS (SCLERODERMA) WITH CARCINOMA
This patient was a man aged 59 who had once been a prize fighter. After stopping this occupation he became a chronic alcoholic. Four years before his death he had haematemesis and melaena on several occasions from a duodenal ulcer. His final admission resulted from increasing breathlessness of 12 weeks’ duration, finally limiting his walking distance to 15 yards. There was also evidence to scleroderma. He died after 6 weeks in hospital. At postmortem an oesophageal stricture was present, there was scleroderma, most evident in the hands, and there were occasional spider naevi.
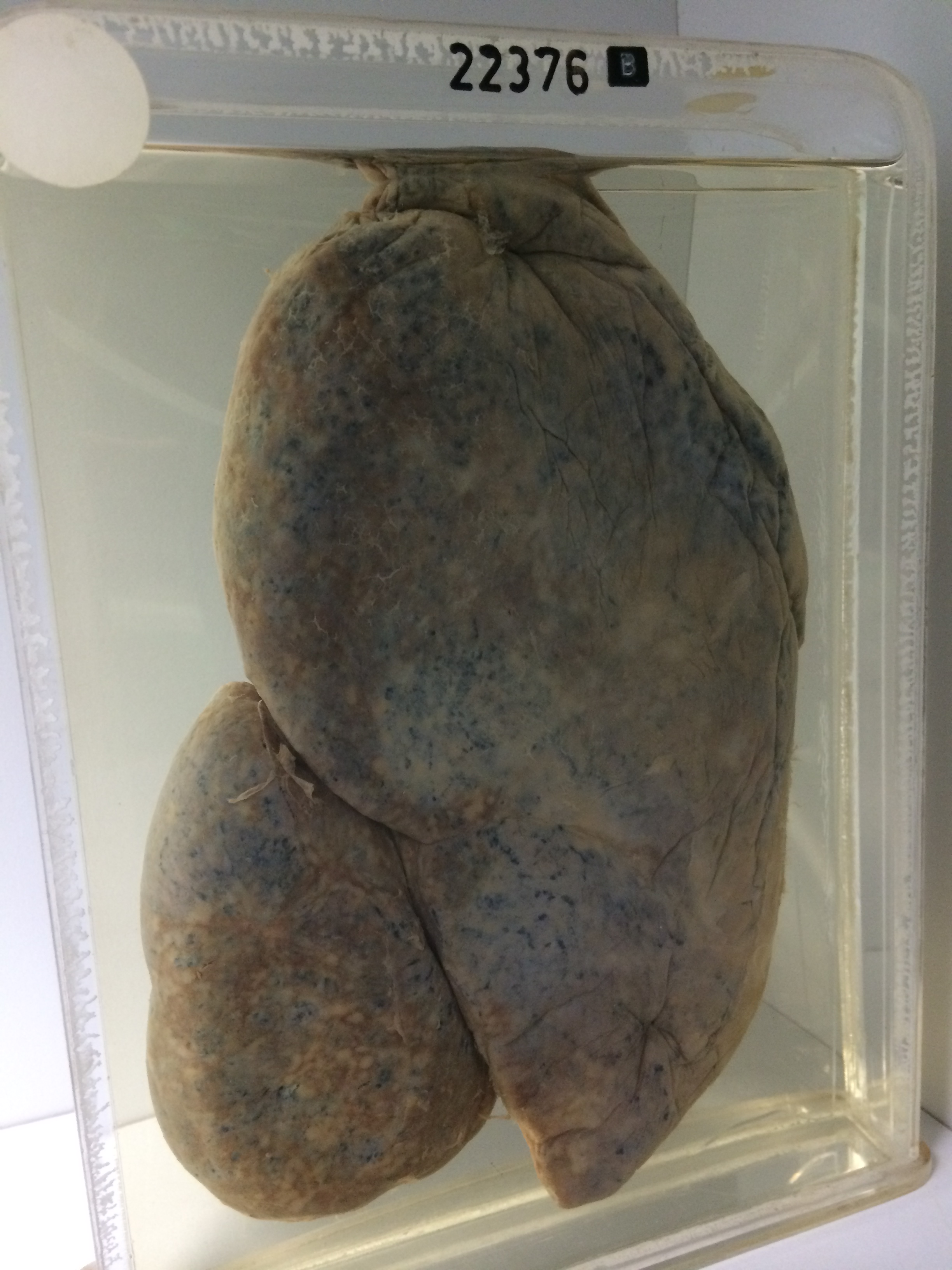
The specimen consists of two portions of the left lung mounted in separate jars. Specimen A shows the cut surface to the front. There is moderate focal centrilobular emphysema with anthracosis is most evident in the upper half of the lung field. There is some stellate increase of interlobular fibrous tissue. The lower lobe is collapsed, fibrous and grey with crowding of bronchi and vessels. The fibrosis is most marked in a thick band some cms deep beneath the pleura. Specimen B is mounted with the pleural surface to the front. Fibrinous and slightly haemorrhaging pleural reaction is evident and small yellow rounded neoplastic deposits are very evident beneath the congested pleura of the collapsed and fibrous lower lobe. Similar neoplastic deposits are also present in the upper lobe near the interlobar fissure. There is some fibrous and fibrinous pleural reaction over the anterior aspect of the upper lobe. Histology shows diffuse interstitial fibrosis with cyst formation and patches of acute bronchopneumonia. The tumour is a columnar mucin-secreting multifocal adenocarcinoma.