25671 MUCIN-SECRETING CARCINOMA, EMPHYSEMA AND SILICOSIS
The patient was a man aged 50 who presented with pain in the left chest, worse on coughing and deep breathing. Alveolar cell carcinoma of the lung had been diagnosed ten months previously. He had been treated for pulmonary tuberculosis 3 years ago and had been exposed to silica for 7½ years commencing about 30 years ago. He was given radiotherapy, but died after about a month.
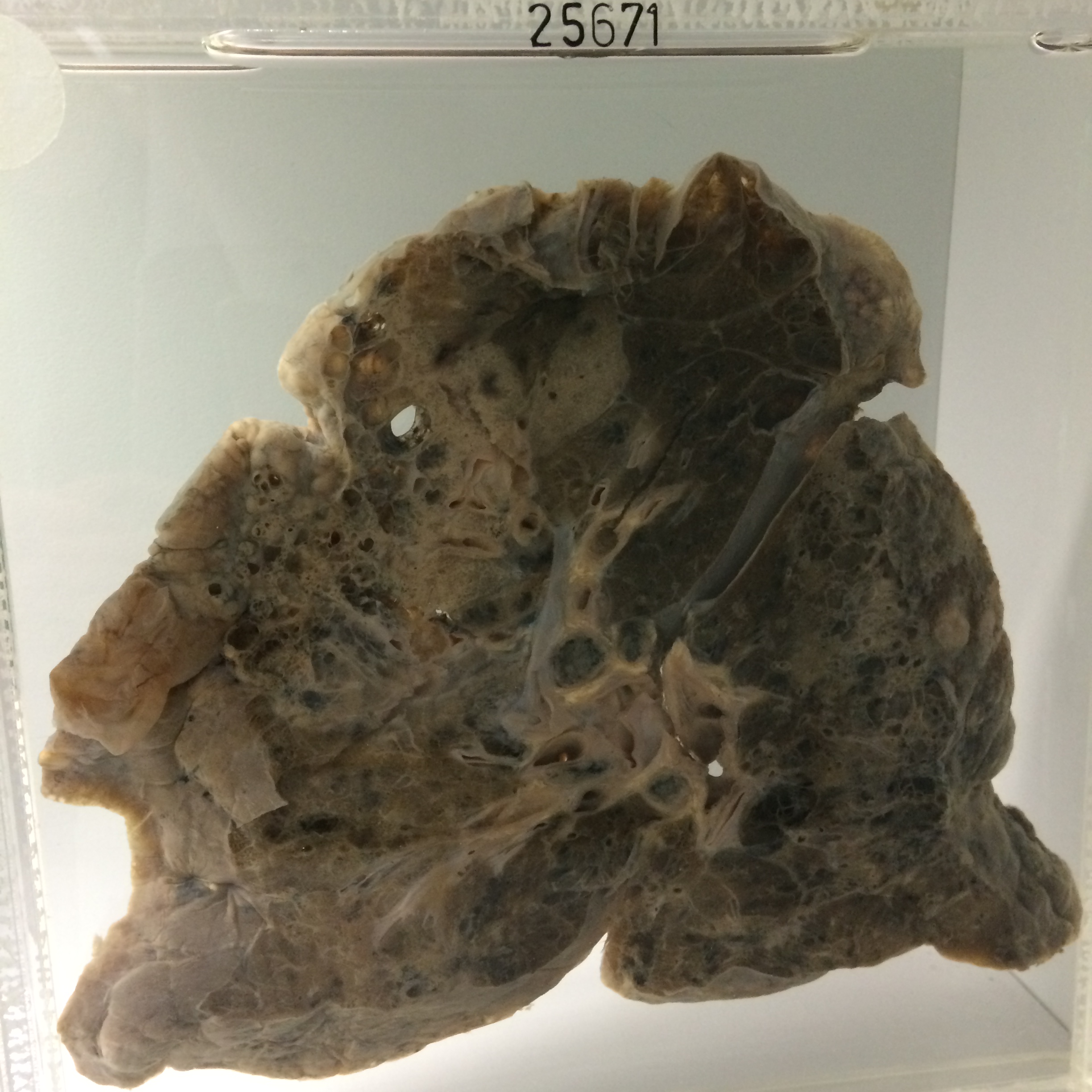
The specimen consists of a slice of the left lung divided in the sagittal plane. There is very marked destructive panlobular emphysema maximal at the apex, and in the posterior zone of the upper lobe, and along the posterior border of the lower lobe. In the latter situation there is what appears to be purulent exudate in dilated air spaces. There is a large zone of mucinous consolidation in the lingular segment of the upper lobe, involving emphysematous air spaces and bullae. Hilar nodes are anthracotic and are slightly enlarged. There is a more solid area of peribronchial tumour in the hilar region of the lower lobe. Histology shows mucin-secreting carcinoma in which tumour cells occur along alveolar walls and the alveoli are filled with mucin. In some areas the tumour is less differentiated, and of the large-cell anaplastic type, and in yet other areas there is some squamous differentiation. Patchy areas of bronchopneumonia and lipid pneumonia are present adjacent to the tumour. At the base, in the anterior basal segment of the lower lobe and in the adjacent segment of the upper lobe, are areas of fibrous scarring.