10295 GRANULOMATOUS MYOCARDITIS
The patient was a women aged 38. Four months previously she had consulted her local doctor because of pain in the right side and the back. X-ray showed early osteoarthritic changes in the spine and she was given butazolidine in large dosage. Six weeks later she developed nausea and vomiting with hepatomegaly and an erythematous skin rash. On admission to Northfield Infectious Diseases Hospital she was diagnosed as butazolidine poisoning. Two weeks after admission she was discharged and seemed to be improving at home, but then became very tired, vomited, and there was breathlessness and retrosternal constriction. On examination there were faint distant heart signs, an impalpable pulse (rate 110) and the liver and enlarged 4 fingers and tender. She did not improve and died. At postmortem there was desquamation of the skin and excess of clear fluid in the pericardial sac and an enlarged liver with a mottled appearance. The spleen was enlarged and congested.
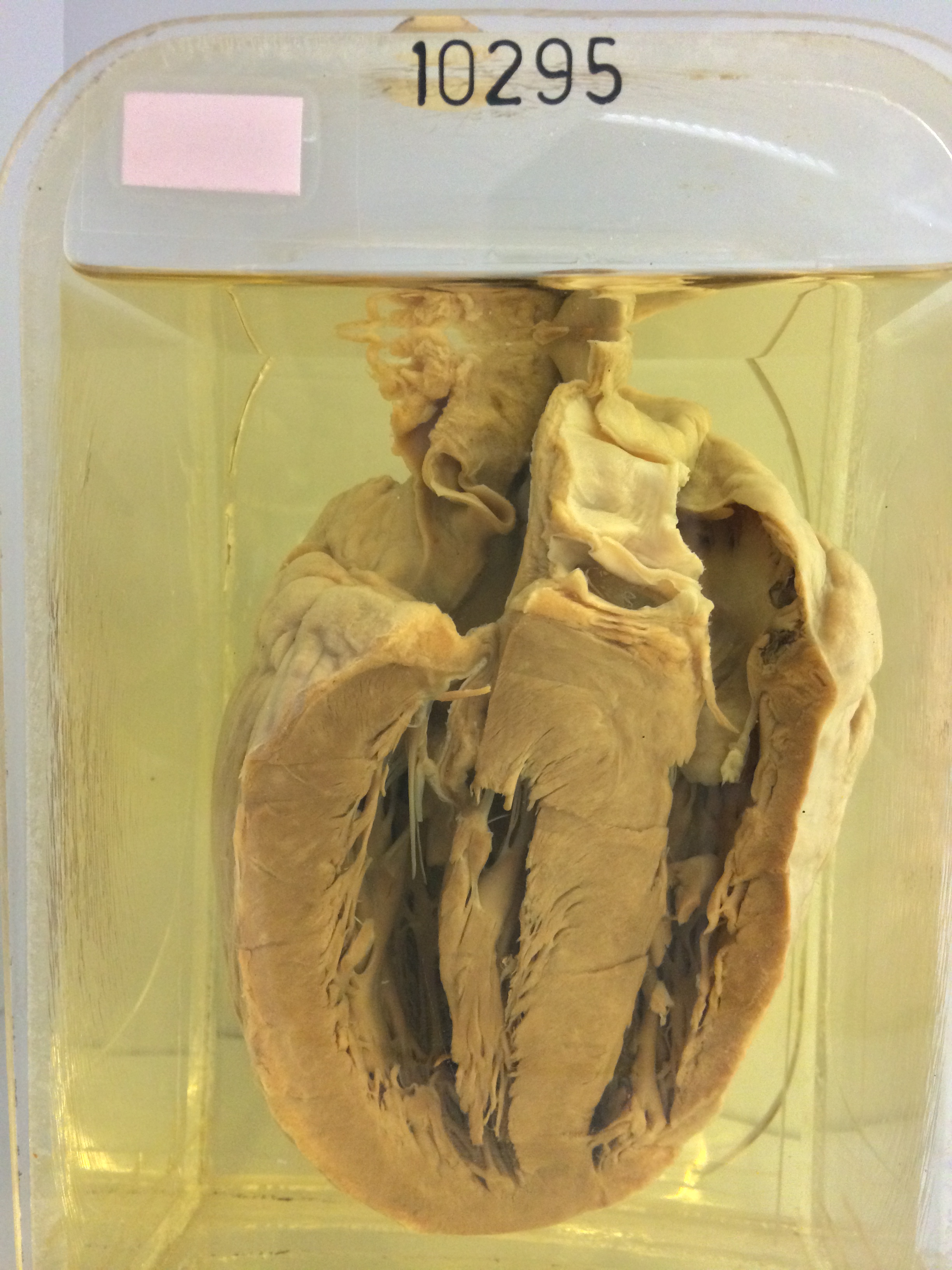
The specimen is the heart sectioned to show ill-defined pale mottling of the myocardium of both left and right ventricles. Histology shows very extensive myocarditis. In many places the myocardium is almost completely destroyed and there is a dense inflammatory infiltrate consisting of lymphocytes, plasma cells, macrophages, many eosinophils and some giant cells. Similar granulomata are present in the liver, mainly in the portal tracts.