25299 MULTIFOCAL ADENOCARCINOMA WITH SPREAD TO PLEURA, PERICARDIUM AND MEDIASTINUM
The patient was a man aged 48 who had been a heavy smoker for many years, but ceased to smoke 13 weeks before his last admission, because of increasing exertional dyspnoea associated with cough, sputum and pain in the left posterior chest. He was given antibiotics by his local doctor without improvement. After 3 weeks the cough had become much worse, with copious sputum production. Chest X-ray then showed extensive consolidation throughout the left lung with an overlying pleural effusion. Twenty five years previously he had pulmonary tuberculosis which was treated with streptomycin. While in hospital the left pleural effusion was repeatedly aspirated and showed adenocarcinoma cells on two occasions. He was given cytotoxic drugs but gradually declined and died after a month in hospital.
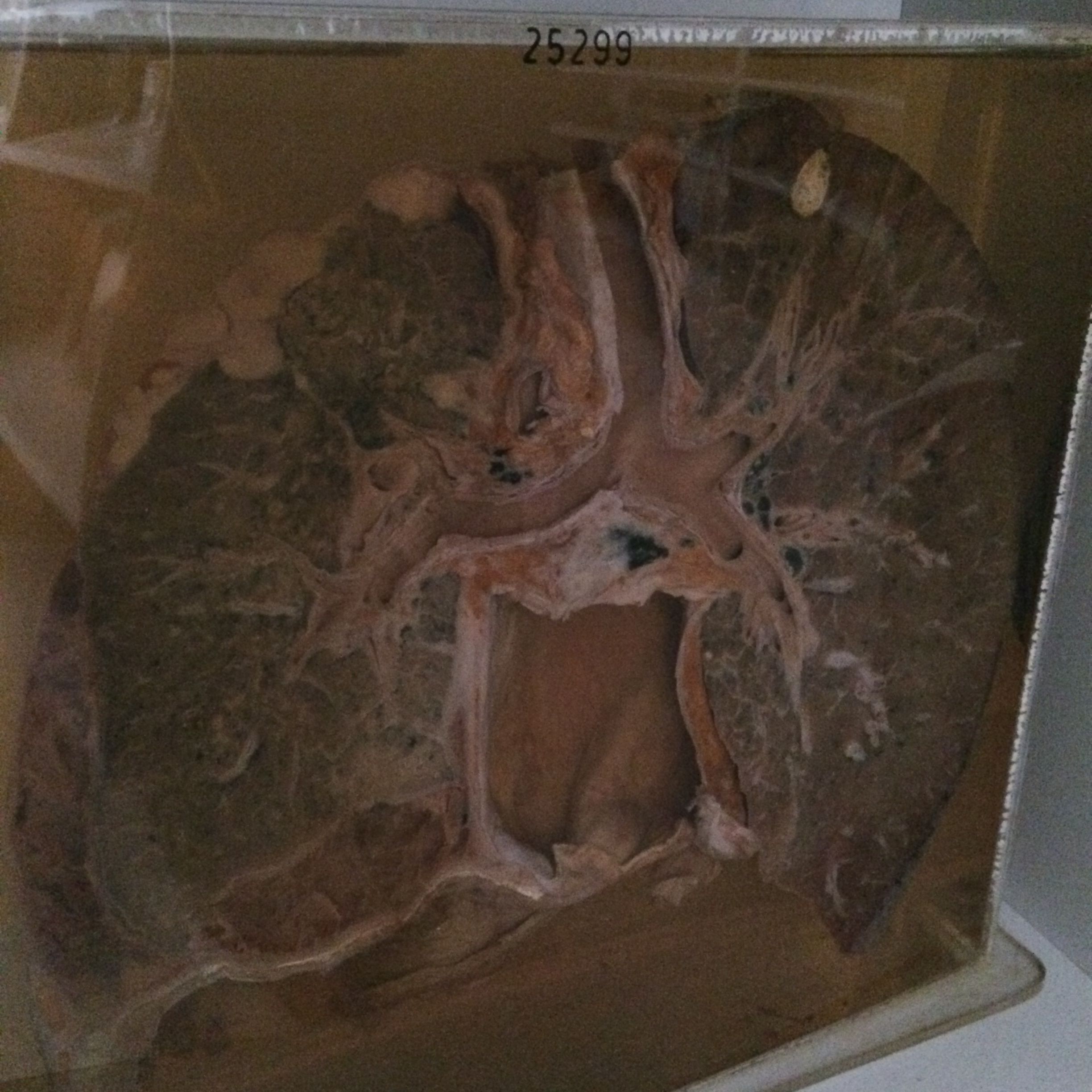
The specimen consists of the lungs, left pleural cavity, pericardium and main respiratory passages sectioned in the coronal plane. There is a thick nodular fleshy layer of white neoplasm covering the apical and lateral aspect of the left upper lobe to a maximum depth of 2 cms. Many small deposits of tumour about 3-4 mms in diameter are scattered throughout the remainder of the left lung, and there is a nodular mass of tumour in the lateral costophrenic angle. Above this there is a loculated fibrinous pleural effusion covering the inferior and lateral aspects of the lower lobe which is partially collapsed. The right lung shows an old inactive encapsulated inspissated tuberculous focus 2 x 1.5 cms at the apex and some malignant lymphatic permeation in the medial aspect of the lower lobe against the pericardium. There is marked malignant infiltration of the entire anterior surface of the parietal pericardium. This is best seen on the reverse of the specimen. Histology shows tubular and solid-acinar adenocarcinoma growing in nodular masses and within alveoli. Permeation of lymphatics in thickened interlobular septa is prominent. There are widespread bronchopneumonic patches.