24869 RUPTURE OF AORTA WITH FALSE ANEURYSM
The patient was a woman aged 80 who was admitted with a 2 month history of breathlessness, ankle swelling and episodic central chest pain. There was a cough productive of white sputum. She had been receiving digoxin and a diuretic. The B.P. was 115/90 and there was auricular fibrillation. Chest X-ray showed a large left bilar opacity. A few days later she developed a left pleural effusion which was at first attributed to pulmonary embolism, but tomography showed a dissecting aortic aneurysm which was increasing in size. She died after 16 days in hospital. At postmortem there was a straw-coloured left pleural effusion measuring 800 mls which was separated by a single layer of parietal pleura from a large haematoma lying above and medial to the left upper lobe. The heart was slightly enlarged (320 gms).
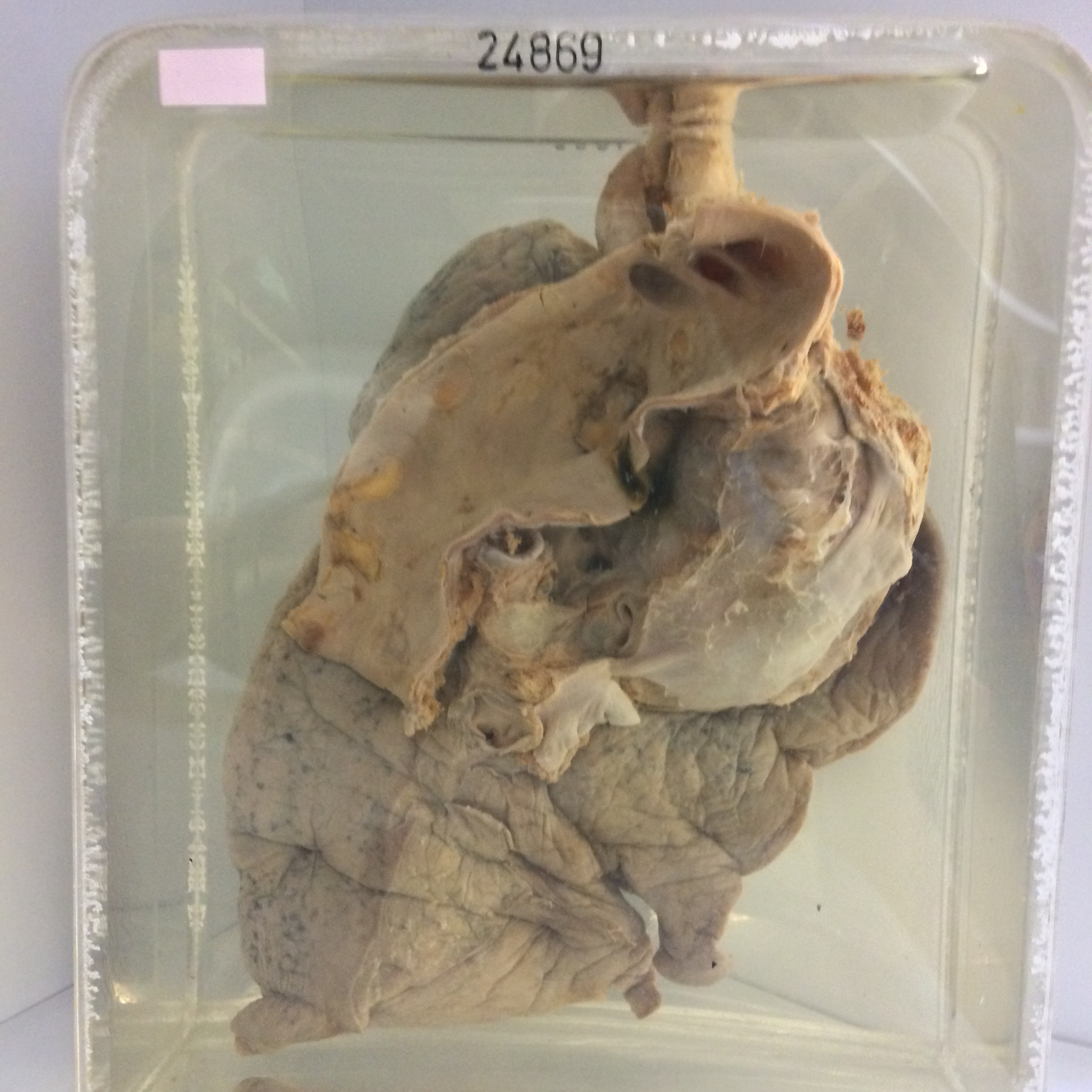
The specimen consists of the descending portion of the arch of the aorta and the origins of the great vessels. An ovoid defect measuring 2.5 x 1.5 cms lies on the anteriolateral wall of the aorta 3 cm distal to the origin of the left subclavian artery. This defect has originated in a split at the margin of a calcified atheromatous plaque and a globular false aneurysm 8 cm in diameter, entirely filled with antemortem thrombus, is adherent to and compresses and distorts the anterior segment of the left upper lobe. This haematoma has ruptured through a large oval defect on its anterior aspect to produce the retropleural haematoma found at postmortem. Inferiorly the sac extends to the hilum and left main bronchus is displaced slightly downwards, along with branches of the pulmonary artery.