22945 CARCINOMA OF LUNG WITH EXTENSION TO CERVICAL NODES
The patient was a man aged 78 who had an influenzal illness for one month followed by cough and mild haemoptysis. There had been loss of weight for two months. Chest X-ray showed an opacity in the left apex and malignant cells were found in one of many sputum specimens. He died after 3 months.
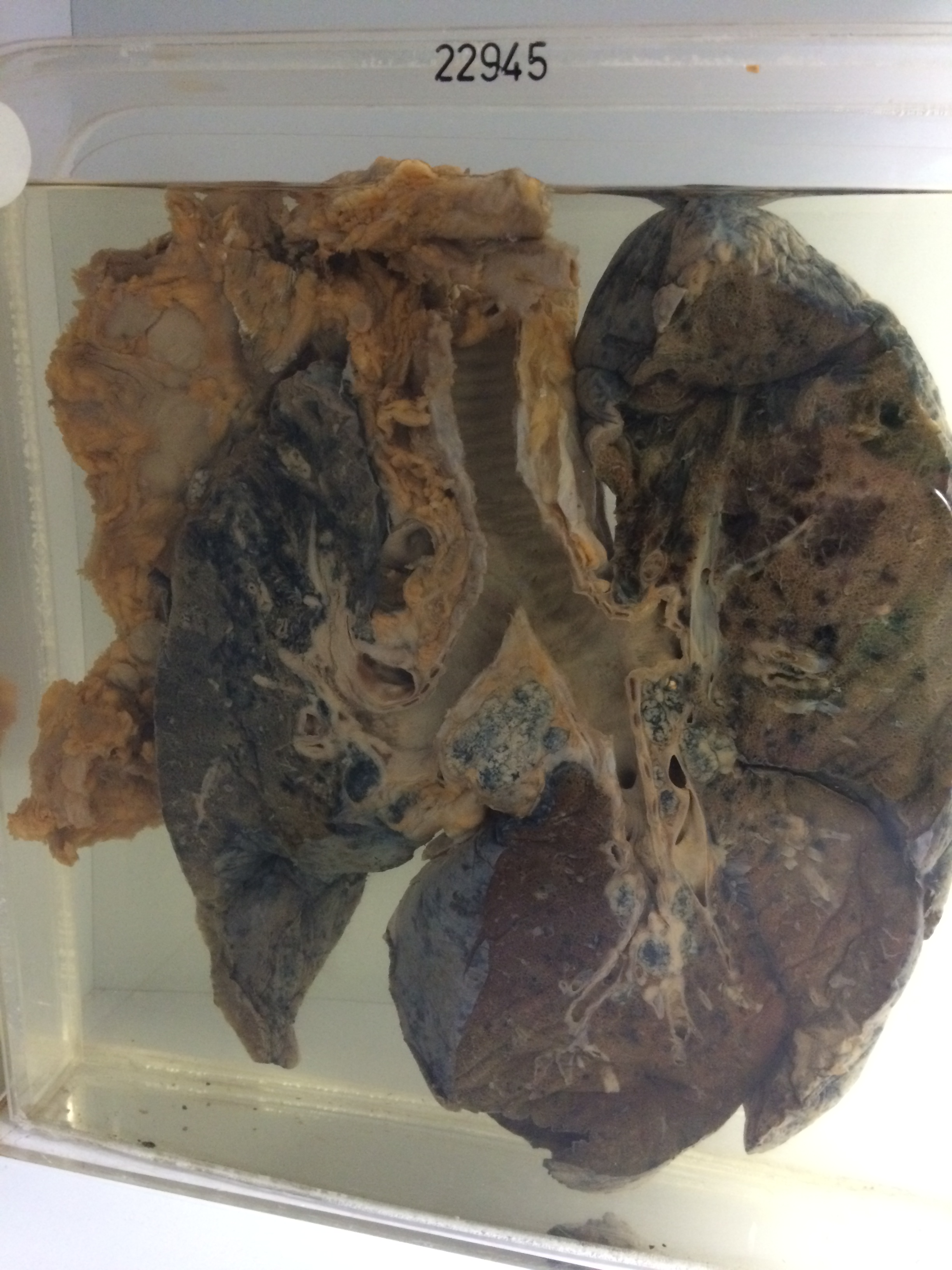
The specimen consists of the lungs and main respiratory passages sectioned in the coronal plane. There is a primary carcinoma arising from the man stem bronchus to the left upper lobe. The lung distal to the tumour shows marked anthracosis and chronic destructive pan-lobular emphysema. Nodules of lymph-spread tumour are also present. The left apex is adherent to the dome of the pleura and there are large involved lymph glands in the lower supra-clavicular region. The right lung shows marked destructive panlobular emphysema with anthracosis at the apex, where there is a small nodule of tumour about 1 cm x 4 mms lying immediately beneath the pleura. There are many involved nodes around the main bronchus to the lower lobe, with some extension through the bronchial wall to produce mucosal nodules. However these nodules are not ulcerated except in one place. There is a further small patch of tumour lying far out beneath the pleura on the lateral aspect of the right middle lobe. There are many involved nodes around the right main bronchi and beneath the bifurcation of the trachea. There is antemortem thrombus without infarction in medium sized vessels in the hilar aspects of the right upper lobe. There is a small calcified tuberculous focus 3 mms in diameter in a lymph node lying above the bronchus to the right lower lobe. This node also contains secondary carcinoma. Histology shows a columnar-celled adenocarcinoma.