25611 BACTERIAL ENDOCARDITIS - MITRAL VALVE PROSTHESIS
The patient was a women aged 50 who first presented in April 1976 with a cardiac murmur, increasing breathlessness and hypertension despite medication. Investigation showed mitral and aortic stenosis and both valves were replaced in May 1977 with a history of night sweats, general malaise and loss of weight. Blood culture grew diphtheroids. She was treated with prednisolone and diuretics, but right and left heart failure increased. Both valves were replaced again. The original mitral prosthesis was covered by vegetations. After operations intensive care was needed for increased cardiac failure, but she improved and was discharged. She was readmitted in September 1977 with a two-week history of lethargy, increasing heart failure, and occasional fever up to 38 degrees Celsius. She died suddenly on the day of admission.
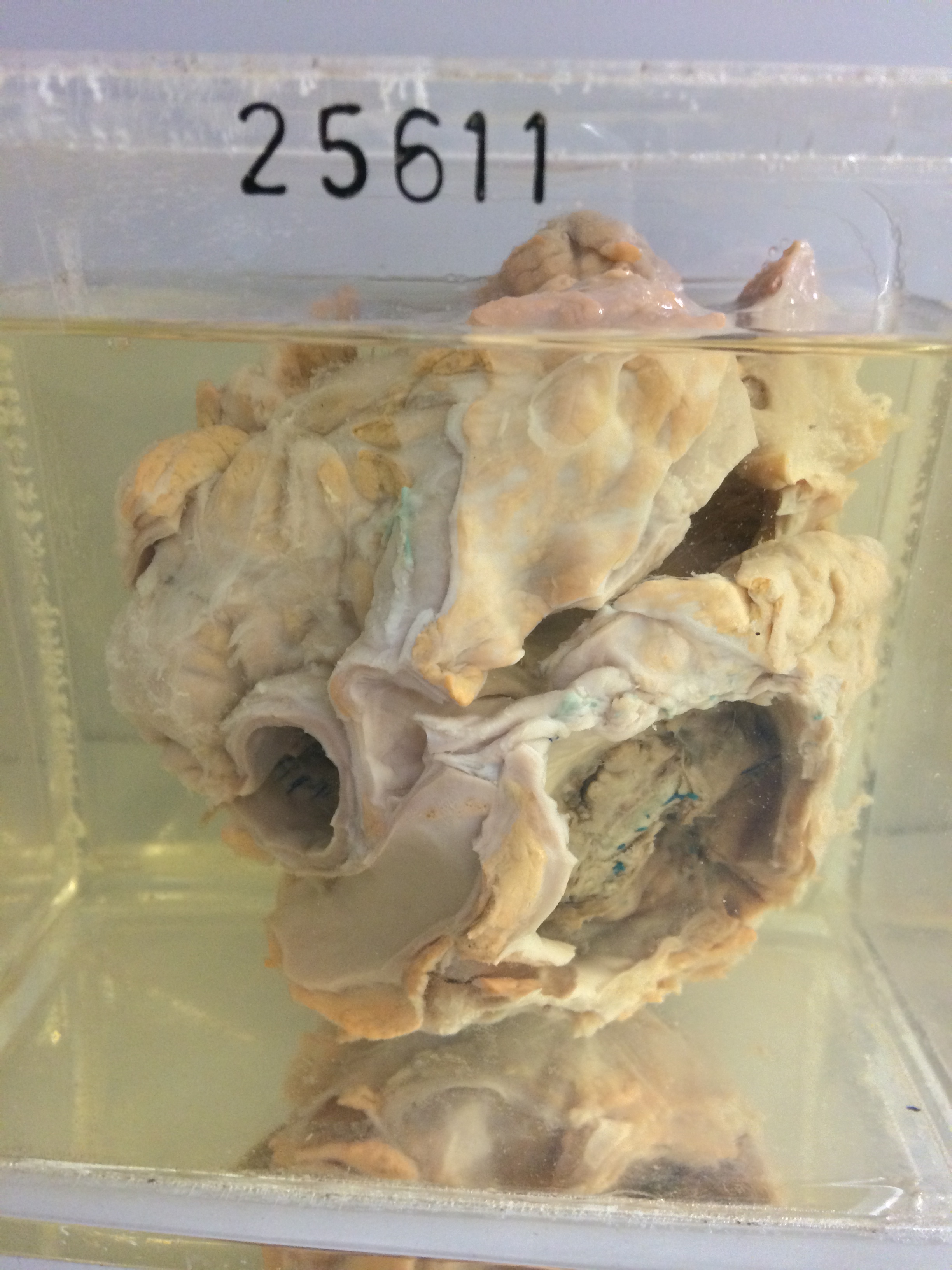
The specimen is the heart mounted to be viewed from the rear. The left atrium is not dilated, but the wall is somewhat hypertrophied and shows patchy fibrosis. The endothelium of the atrium is wrinkled and thickened. A large firm fibrinous vegetation infiltrated with blood is present on and around the mitral valve prosthesis. Surgical sutures are visible embedded in the substance of the vegetation. The orifice of the valve is considerably narrowed, measuring only some 6 x 6 mms. The left ventricle is not dilated or hypertrophied. The tricuspid valve is dilated but is not diseased. The aortic valve prosthesis is firmly seated, but there is a small amount of fibrinous vegetation present around the margin of the aortic prosthesis, particularly anteriorly. Histology shows the vegetation to be composed of dense fibrin containing very numerous large masses of gram positive cocci. There are scantly collections of leukocytes. The wall of the left atrium is a little edematous, but there are no special inflammatory changes.