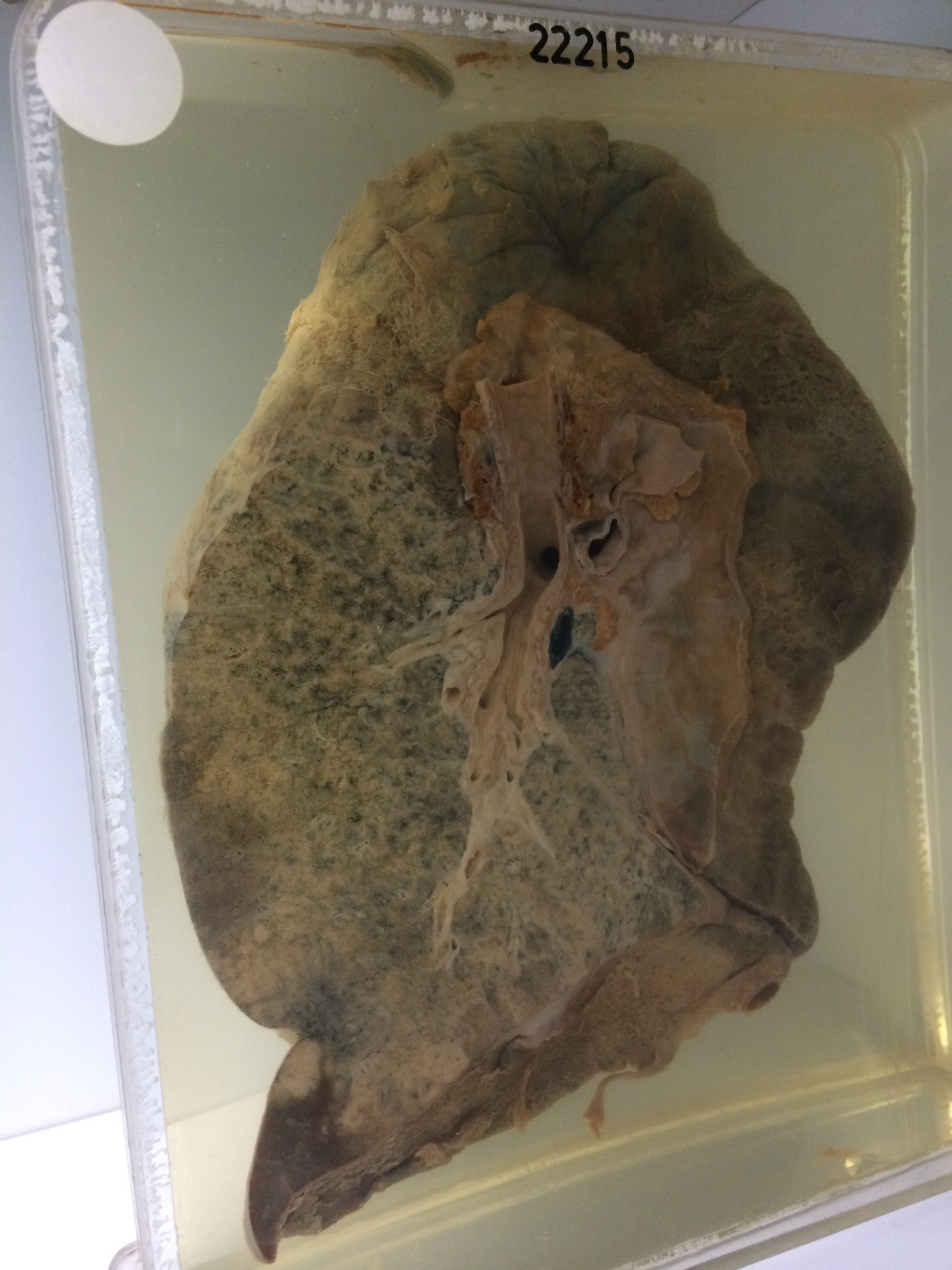
22215 CARCINOMATOSIS WITH BRONCHOPNEUMONIA
This patient was a man aged 59 who was referred from the chest clinic because of a radiological opacity in the left lower lobe which had not been present two years previously. He had also had small haemoptyses for the last 3-4 days. There were clinical signs of consolidation in the left lower lobe with overlying effusion. Two aspirations were performed, yielding 1500 mls of blood-stained fluid. cytology of the sputum and pleural fluid was positive for malignant cells and bronchoscopy showed rigidity and narrowing of the left lower lobe bronchus. He died after two weeks in hospital before radiotherapy was begun.
The specimen consists of the left lung which shows scattered confluent pale neoplastic areas and scattered areas of bronchopneumonia, together producing almost complete consolidation of the lower lobe. The major bronchi are clear and there is no obvious localised tumour mass. There are some areas o haemorrhagic necrosis and old infarction towards the periphery of the lobe. A similar appearance is present in the hilar and lingular aspects of the upper lobe. There is a diffuse marked fibrinous pleurisy. Hilar nodes are not obviously involved. There is an area of neoplastic thickening of the main stem bronchus extending over a distance of about 2 cms without obvious diminution of the lumen. The appearance suggests diffuse carcinomatosis of the lung with superimposed bronchopneumonia and patchy infarction. At postmortem tumour was present only in the left lung and there were no distant metastases. Histology shows a slightly anaplastic carcinoma in which squamous features predominate.