24774 DIFFUSE PRIMARY ADENOCARCINOMA
The patient was a man aged 69. Six months previously he sustained concussion and fractured ribs, scapula and pelvis in a car crash. On the last occasion he was admitted with breathlessness for 3 days, constant pain across the upper chest, poor appetite with recent weight loss, slight fever and a non-productive cough. On examination there was a right basal pleural effusion. Chest X-ray showed diffuse opacities in the lungs as well as the effusion in the pleural cavity. There was a microcytic anaemia and the sputum was suspicious for malignant cells. Bone marrow biopsy showed adenocarcinoma. Fever continued with a rising leucocytosis and the sputum grew a Klebsiella. He continued to deteriorate, developed congestive cardiac failure with enlargement of the liver and died after a month in hospital. At postmortem there were widespread tumour deposits in lungs, pleura, mediastinum, liver, mesentery, peritoneum, prostate and bone marrow.
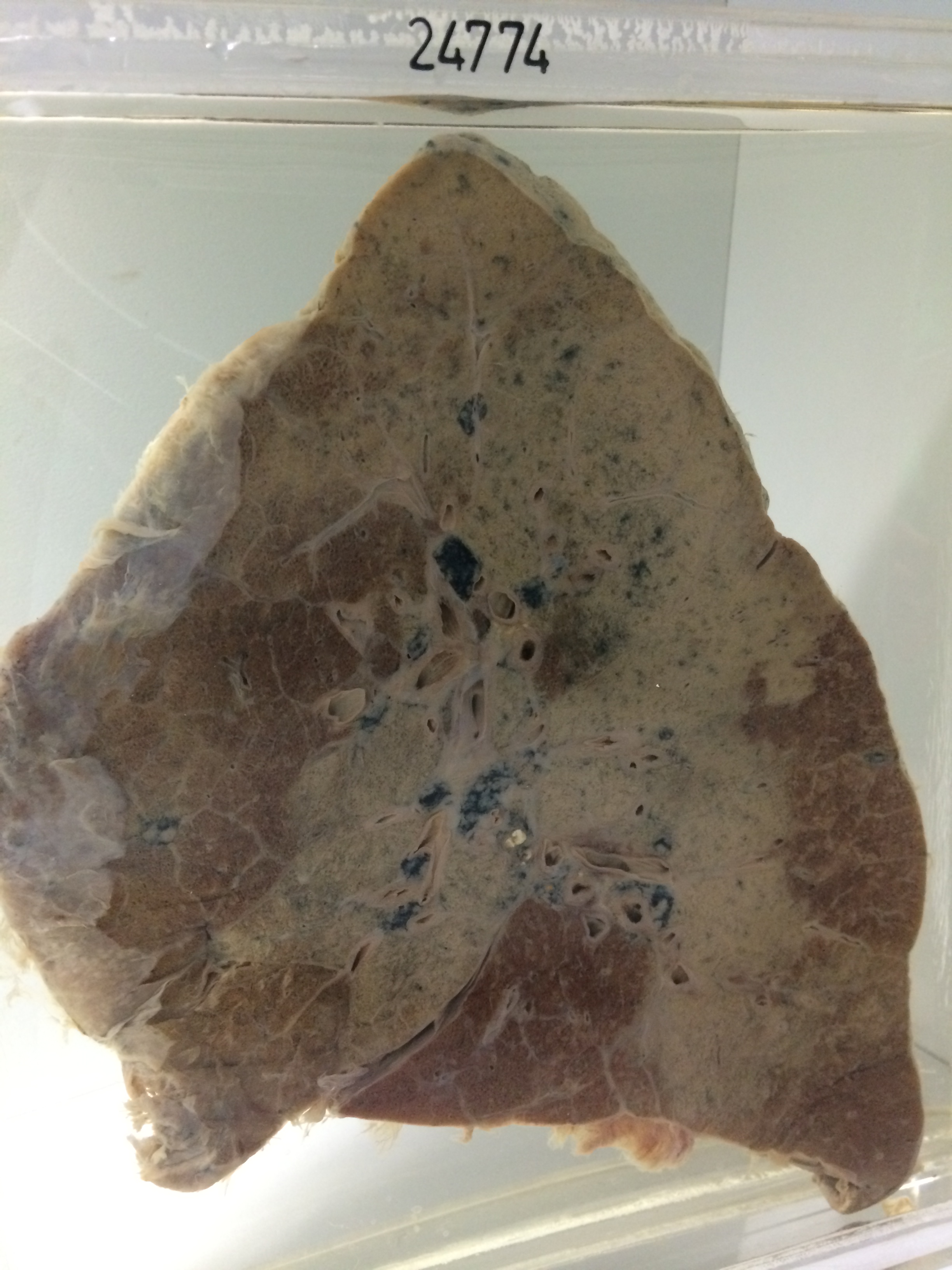
The specimen consists of the right lung sectioned to show widespread grey consolidation. From the apical segment of the upper lobe this consolidation extends to involve the posterior segment and has spread across the interlobar fissure into the lower lobe and into the hilar aspects of the middle lobe. The remainder of the lung shows some exaggeration of interlobular septa and tiny pale miliary nodules of tumour are visible in the posterior segment of the lower lobe in the region beneath the pleura. The overlying pleura shows fibrous and fibrinous reaction. There is an old tuberculous calcification in a lymph node at the hilum. Histology shows a tubular cuboidal celled adenocarcinoma growing profusely within lung alveoli. In the lower lobe there is permeation of perivascular and interlobular lymphatics as well as patchy acute bronchopneumonic consolidation.